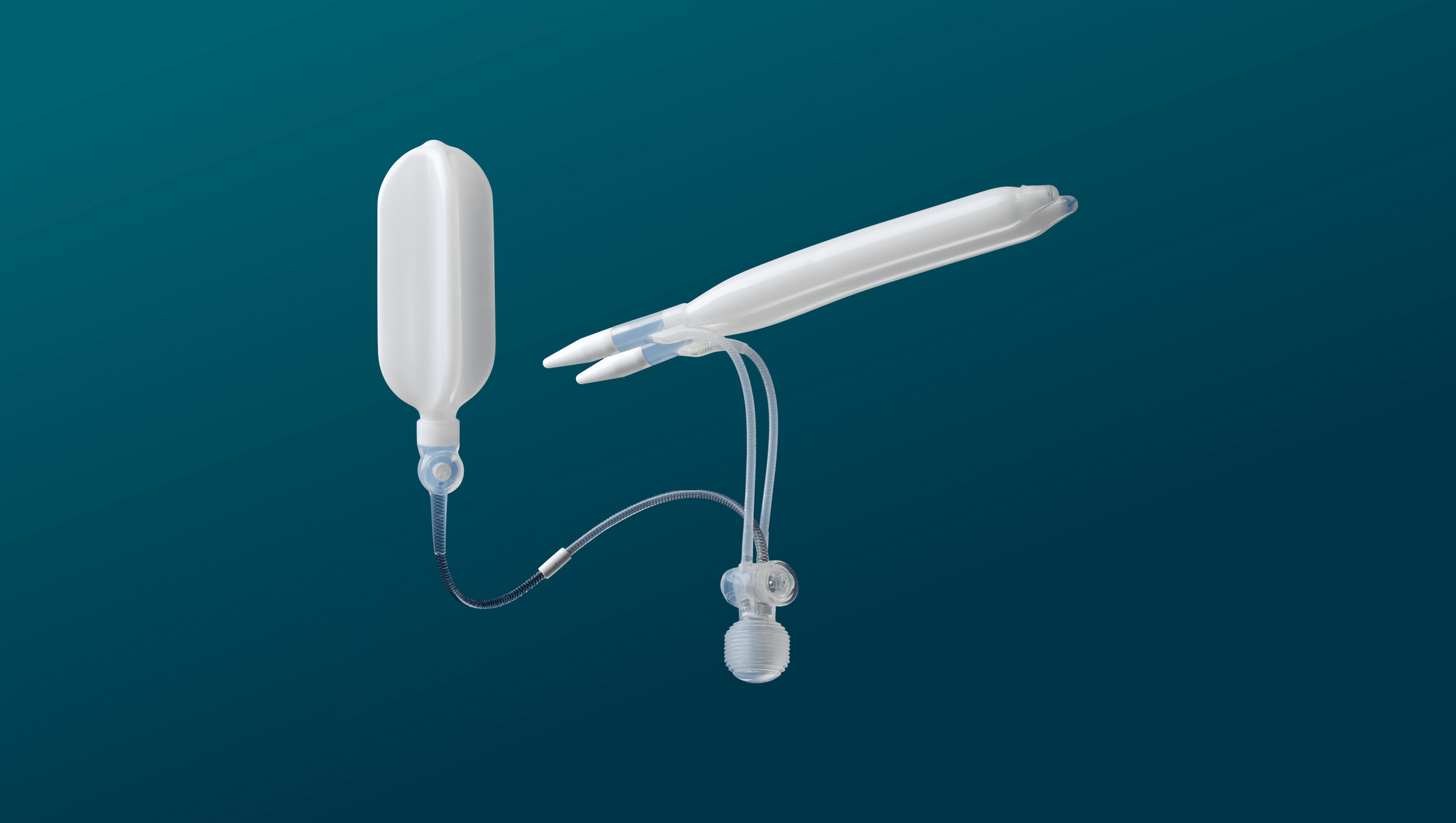
An inflatable penile implant works on a single physical action: a squeeze. A few presses on a small pump hidden inside the scrotum move sterile fluid from a reservoir into two cylinders placed inside the penis, and within seconds rigidity returns. After intercourse, a release button on the same pump sends the fluid back, and the penis returns to its natural soft state. This is the closest mechanical replication of a normal erection that current medicine offers, and it happens entirely inside the body with nothing visible from the outside.
The three-piece inflatable is the device we reach for when erectile dysfunction has stopped responding to medications and injections. It is also the implant we recommend when a patient prioritizes a natural flaccid state, full concealment under everyday clothing, and the ability to choose when an erection happens rather than living with one continuously. The trade-off is a learning curve with the pump, and confidence with that sequence builds over the first few weeks of use.
This guide covers what the three-piece system is, which patients genuinely benefit from it, the specific models we implant at Istanbul Urology Clinic, and the realities patients only hear about once they sit down in consultation. The inflatable is the default choice in severe ED for a reason, but it is not the right choice for everyone, and the difference matters more than patients expect.
- What an Inflatable Penile Implant Actually Is
- The Patients Who Actually Benefit From an Inflatable
- How the Three Pieces Work Together
- The Squeeze: How Activation Actually Happens
- What Changes and What Doesn't
- The Models We Implant
- Which Implant Do We Recommend Most Often?
- The Length Recovery Option
- What Patients Actually Worry About Before Surgery
- What About Two-Piece Inflatable Implants?
- From Operating Room to First Activation
- A Real Patient Story
- Risks Worth Understanding
- How Long Does an Inflatable Implant Actually Last?
- When Inflatable Is the Clear Choice
- Conclusion
- What an Inflatable Penile Implant Actually Is
- The Patients Who Actually Benefit From an Inflatable
- How the Three Pieces Work Together
- The Squeeze: How Activation Actually Happens
- What Changes and What Doesn't
- The Models We Implant
- Which Implant Do We Recommend Most Often?
- The Length Recovery Option
- What Patients Actually Worry About Before Surgery
- What About Two-Piece Inflatable Implants?
- From Operating Room to First Activation
- A Real Patient Story
- Risks Worth Understanding
- How Long Does an Inflatable Implant Actually Last?
- When Inflatable Is the Clear Choice
- Conclusion
Key Points
- A three-piece inflatable penile implant restores erections on demand through a fully internal hydraulic system, with no external components visible at any time.
- It is the closest mechanical replication of a normal erection currently available, and the only treatment that allows control over both inflation and full deflation.
- Patients who fail oral medications, injections, and vacuum devices are candidates, particularly when concealment and a natural flaccid state matter for daily life.
- Modern three-piece systems from AMS, Coloplast, and Rigicon are engineered for 15 to 20 years of reliable function, with patient satisfaction reaching 92.4% in recent clinical studies (Karaman et al., 2025).
- Two models, the AMS 700 LGX and the Rigicon Infla10 AX, support gradual length recovery of 1 to 3 cm over 6 to 12 months with consistent post-operative cycling.
- Surgery takes 45 to 90 minutes, requires one night of hospital observation, and intercourse is cleared at the six-week mark after device activation.
What an Inflatable Penile Implant Actually Is
A three-piece inflatable penile implant is a fully internal hydraulic system that replaces the function of the spongy erectile tissue inside the penis. Two cylinders sit along the length of the corpora cavernosa, a pump is concealed inside the scrotum, and a small reservoir holding sterile saline rests behind the lower abdominal muscle. The three components are connected by thin internal tubing, and the entire system stays inside the body permanently after surgery.
This is what makes it mechanically different from every other implant category. A malleable implant produces rigidity through a bendable metallic core that is always firm. An inflatable produces rigidity on demand. When the pump is not activated, fluid sits in the reservoir, the cylinders stay empty, and the penis returns to a soft flaccid state that looks and feels close to natural. When the pump is squeezed, fluid moves into the cylinders, the penis becomes firm, and intercourse becomes possible. The state of the penis is no longer determined by blood flow or vascular health. It is determined by whether the pump has been activated.
This shift is the reason the three-piece inflatable is considered the gold standard for severe erectile dysfunction. It removes vascular ED, diabetic vasculopathy, post-prostatectomy nerve damage, and Peyronie’s-related dysfunction from the equation entirely, while preserving the natural flaccid appearance men with active professional and social lives need. The trade-off is mechanical complexity: a learning curve with the pump, and a small long-term risk of mechanical wear after fifteen or twenty years of daily use.
The Patients Who Actually Benefit From an Inflatable
The inflatable penile implant is not the right device for every patient with erectile dysfunction. It is the right device for specific clinical and lifestyle situations where the combination of on-demand rigidity, full deflation, and complete concealment delivers something no other implant can match. Three patient profiles consistently make up the majority of inflatable cases at our clinic.
1. Younger and Sexually Active Patients
Men in their forties, fifties, and early sixties who are still sexually active and prioritize a natural daily experience are the clearest candidates for an inflatable. The reason is daily life, not surgery itself. A malleable implant keeps the penis in a permanent semi-rigid curve, which works mechanically but never disappears under thin clothing or during physical activity. An inflatable returns to a soft flaccid state when deflated, which means the patient lives the rest of the day without a constant physical reminder that something is different.
2. Patients With Active Professional or Social Lives
Businessmen, executives, frequent travelers, and men whose work involves changing rooms, gym memberships, swimming, or any environment where the body is visible to others almost always do better with an inflatable. Concealment is the single most underestimated factor before surgery, and the one patients most consistently mention as a quality-of-life improvement after recovery.
3. Patients Who Failed Medications, Injections, and Vacuum Devices
The standard treatment ladder for erectile dysfunction starts with oral medications, moves to intracavernosal injections if pills stop working, and then offers vacuum erection devices. When all three have failed, the inflatable penile implant is the next step. This is the largest group we see in consultation: men with diabetic vasculopathy, post-radical-prostatectomy nerve damage, severe venous leak, or long-standing erectile dysfunction where the vascular mechanism is no longer recoverable. For these patients, the inflatable does not replace medication. It replaces the vascular event entirely.
Patients outside these three profiles, particularly older men with reduced hand function, severe corporal fibrosis, or those who prioritize mechanical simplicity above everything else, are usually better served by a malleable implant. That decision framework is covered in detail in our Malleable Penile Implant guide.
How the Three Pieces Work Together
| Component | Where It Sits | Why This Design Matters |
|---|---|---|
| Cylinders | Inside the corpora cavernosa, along the full length of the penis | Replaces the erectile tissue function entirely. When filled with fluid, they produce rigidity strong enough for intercourse. When empty, the penis collapses into a natural flaccid state. |
| Pump | Concealed inside the scrotum, between the testicles | Gives the patient full control over inflation and deflation. The position is anatomically discreet and accessible with one hand, even in clothing. |
| Reservoir | Behind the lower abdominal muscle, in the space of Retzius | Stores the sterile fluid invisibly when the implant is deflated. This is what allows the penis to look and feel naturally soft when not in use, unlike simpler implant designs. |
The Squeeze: How Activation Actually Happens
Once healing is complete and the surgical team clears the implant for use, the entire system operates through one repeated motion. Patients are taught the sequence during the activation visit, and confidence builds within a few sessions of practice.
 1. Locate the pump. The pump sits inside the scrotum and is easy to find by touch. With practice, the patient identifies it without looking, using thumb and index finger from outside the scrotal skin.
1. Locate the pump. The pump sits inside the scrotum and is easy to find by touch. With practice, the patient identifies it without looking, using thumb and index finger from outside the scrotal skin.
2. Squeeze to inflate. Pressing the pump bulb several times moves fluid from the reservoir into the cylinders. Modern systems reach full rigidity within 6 to 10 squeezes. The penis becomes firm and remains firm for as long as needed.
3. Use as intended. The implant stays inflated throughout intercourse without losing rigidity. Unlike a natural erection, it does not soften after ejaculation, which means duration is controlled by the patient rather than by the body.
4. Deflate after use. A release button or valve on the pump opens the return path. Fluid moves back to the reservoir, the cylinders empty, and the penis returns to a soft flaccid state within seconds.
The learning curve is real but short. Patients typically operate the pump confidently within two weeks of activation, and the motion becomes fully automatic by the second or third month. Diabetic patients or men with reduced hand strength sometimes need additional practice, which is one of the reasons we evaluate hand function carefully before recommending a specific pump system.
What Changes and What Doesn't
The inflatable penile implant restores erections. It does not change most of the other components of sexual function, which is worth making clear because patients often assume otherwise.
| Function | What Changes After Surgery |
|---|---|
| Erection | Restored on demand through the pump. This is the only function the implant directly replaces. |
| Orgasm | Usually unchanged. The orgasmic pathway is neurological and not affected by implant placement. |
| Sensation | Usually unchanged. Penile skin and glans sensitivity continue to function normally after recovery. |
| Ejaculation | Depends on the underlying condition. If ejaculation was normal before surgery, it usually remains normal. Pre-existing issues like retrograde ejaculation after prostate surgery are not corrected by the implant. |
| Libido | Unchanged directly. The implant does not raise or lower hormonal sex drive. |
| Fertility | Unchanged. The implant is placed in the corpora cavernosa and does not interfere with the urethra, testicles, or sperm pathway. |
Some patients experience indirect improvements that surprise them. A subset report mildly delayed ejaculation after implant surgery, which often improves intercourse duration without requiring medication. Libido frequently increases over the first year, not because of the device, but because the psychological burden of erectile uncertainty is gone. When intimacy stops being a source of anxiety, desire often returns to levels patients had not experienced in years.
The Models We Implant
Three manufacturers dominate the global inflatable market: Boston Scientific (AMS), Coloplast, and Rigicon. At Istanbul Urology Clinic, we maintain the full inflatable line from all three because the right implant depends on anatomy, fibrosis, hand function, and length-preservation goals rather than brand preference alone.
| Brand | Engineering Strength | Best When |
|---|---|---|
| AMS 700 (Boston Scientific) | InhibiZone antibiotic coating, decades of clinical data, three cylinder variants (CX, LGX, CXR) | Standard three-piece cases, length recovery (LGX), tight corporal anatomy (CXR) |
| Coloplast Titan | Bioflex cylinders, strongest axial rigidity, lifetime warranty, Titan Touch one-touch deflation variant | Severe corporal fibrosis, complex Peyronie’s, revision surgery, reduced hand strength (Titan Touch) |
| Rigicon Infla10 | Ergonomic Pulse pump, HydroShield coating, AX expansion cylinders, lifetime warranty | Diabetic or older patients (Pulse), length recovery alternative to LGX (AX) |
Each brand has a dedicated guide covering the specific cylinder behavior, pump options, and clinical use cases in depth. See our AMS 700 guide, Coloplast guide, and Rigicon implants guide for the technical detail.
Which Implant Do We Recommend Most Often?
After thousands of inflatable cases, the same matching patterns appear in our consultations. The implant that fits one patient perfectly is the wrong device for another, and the decision usually maps to one dominant clinical or lifestyle factor.
For length recovery, the choice narrows to the AMS 700 LGX or the Rigicon Infla10 AX. These are the only two implants on the market with bidirectional expansion, and selection between them depends on pump preference and surgeon experience. For severe corporal fibrosis or advanced Peyronie’s, the Coloplast Titan is the consistent choice because Bioflex cylinders handle dense scar tissue better than softer silicone alternatives. For diabetic patients or men with reduced hand strength, the Rigicon Infla10 Pulse and the Coloplast Titan Touch are engineered for easier operation, with the Titan Touch offering one-touch deflation as a distinct advantage.
For tight corporal anatomy or smaller dimensions, the AMS 700 CXR uses narrower cylinders that fit anatomies where standard 3-piece designs are too wide for safe placement. For standard severe ED with no specific complication, the AMS 700 CX or the Rigicon Infla10 Pulse remain the defaults: the CX has the longest clinical track record, the Pulse offers superior pump ergonomics. For patients with prior pelvic surgery making reservoir placement risky, the Rigicon Infla2P two-piece system eliminates the abdominal step entirely.
If we had to name a single default for a typical severe ED case with no specific complication and no length-preservation concern, the answer would be the AMS 700 CX or the Rigicon Infla10 Pulse, depending on whether the patient prioritizes track record or pump ergonomics.
The Length Recovery Option
Many men assume any penile implant restores rigidity but never restores length. This is no longer true. Two devices on the market, the AMS 700 LGX and the Rigicon Infla10 AX, use expansion cylinders that grow in both length and girth during inflation. With consistent post-operative cycling during the first year, the corporal tissue progressively stretches to accommodate the cylinder’s full expansion range.

Patients who follow the cycling protocol gain between 1 and 3 centimeters of length over 6 to 12 months, with an average closer to 2 centimeters. Girth expansion is more predictable and develops earlier, often within the first three months. The improvement depends on tissue elasticity, fibrosis severity, age, and cycling consistency.
This is not the right option for every patient. Severe fibrosis, advanced Peyronie’s, or significant scarring usually do better with rigidity-focused designs like the Coloplast Titan or AMS 700 CX. For men who lost length over years of erectile dysfunction or after radical prostatectomy, an expandable implant recovers dimensions other devices cannot. The full cycling protocol and candidate criteria are in our AMS 700 LGX guide.
What Patients Actually Worry About Before Surgery
After thousands of inflatable penile implant consultations, the same concerns surface once the medical conversation is over and the patient is sitting quietly, thinking about what daily life will actually feel like.
Partner sensation during intercourse. The pump sits inside the scrotum, below and behind the penis, completely outside the path of any sexual activity. Partners do not notice it during intercourse or foreplay.
Accidental activation during exercise. Inflating the device requires deliberate, repeated squeezing of the pump. Tight underwear, sitting, cycling, or gym activity will not move enough fluid to produce an erection.
Feeling the reservoir when bending or sitting. The reservoir is placed behind the lower abdominal muscle in a deep anatomical space. Some patients describe mild awareness during the first few weeks, but this fades by the third month and the reservoir becomes mechanically silent in daily life.
Confidence with pump operation. Patients typically become confident with inflation and deflation within two weeks of activation. The motion becomes fully automatic by the second or third month, similar to typing or driving.
Losing hand strength with age. A legitimate long-term consideration for patients in their sixties or seventies at the time of surgery. Pump choice matters: the Coloplast Titan Touch and the Rigicon Pulse require significantly less hand strength than older pump designs.
The implant feeling like a foreign object. During the first few weeks, yes. By three months, patients describe the implant as feeling like a natural part of their anatomy. By six months, the awareness disappears almost entirely outside of activation itself.
The pattern across all of these concerns is the same. The fear before surgery is almost always larger than the reality after recovery. Patients who give the implant six months of adaptation rarely list any of these worries as significant problems at the one-year follow-up.
What About Two-Piece Inflatable Implants?
The three-piece system is the default for most inflatable cases, but it is not the only option. A two-piece inflatable uses the same hydraulic principle with one engineering difference: the reservoir is built into the cylinders themselves rather than placed separately behind the abdominal muscle. Two components are implanted instead of three, and no abdominal space is required.

This matters in specific clinical situations. Patients with prior radical prostatectomy, major pelvic surgery, kidney transplantation, or extensive abdominal scarring sometimes have a compromised retropubic space where placing a traditional reservoir becomes technically difficult or carries higher risk. In these cases, a two-piece system delivers the core advantage of an inflatable, on-demand rigidity with a soft flaccid state, without requiring a surgical step into the abdomen.
The modern two-piece option we use is the Rigicon Infla2P. It is pre-filled and pre-connected from the manufacturer, which shortens operating time, and uses the same Pulse pump found in the Infla10 series. The flaccid state is softer than older two-piece systems but does not match a three-piece’s full deflation, since fluid storage is more limited. For patients whose anatomy makes a three-piece risky, this is a meaningful upgrade over a malleable while keeping the surgery simpler.
From Operating Room to First Activation
Inflatable penile implant surgery takes 60 to 90 minutes under general or spinal anesthesia, performed through a small incision near the penoscrotal junction. The cylinders are placed inside the corpora cavernosa, the pump is positioned in the scrotum, and the reservoir is tucked behind the lower abdominal muscle. Patients typically spend one night in the hospital for observation and leave the following morning with supportive underwear and a complete medication package.
Recovery follows a predictable arc. Swelling and tenderness peak in the first 72 hours. Office work and light daily activity resume between days 10 and 14, the point at which most international patients fly home. Healing is confirmed at the 4 to 6 week follow-up, when the implant is activated for the first time under guided instruction. Sexual activity is cleared from week 6 onward, and confidence with the pump builds over the next two to three months.
The full week-by-week breakdown, including warning signs, return-to-work timing for different professions, and what the first activation visit looks like, is covered in our Penile Implant Recovery Timeline.
A Real Patient Story
A businessman in his late forties came in convinced he needed a malleable implant after months of online research. The clinical picture told a different story. He had no limitations on hand function, his penile length was around 18 cm, and his lifestyle involved international travel, frequent social events, and a regular gym routine with swimming and sauna use.
We explained that a permanently semi-rigid penis at his length would show under tailored trousers and athletic wear in ways he would notice immediately. The simplicity that drew him to a malleable would become a daily compromise rather than a clinical advantage.
He took several days to think about it and proceeded with an AMS 700 CX inflatable. Six months later, what he valued most was not the rigidity itself, which he expected, but the soft flaccid state during normal daily life.
The right implant is not always the simplest one or the most advanced one. It is the one that matches the anatomy and the life the patient is actually going to live with the device.
Risks Worth Understanding
| Complication | Reality and Frequency |
|---|---|
| Infection | Below 2% in first-time implant surgery when modern antibiotic coatings, sterile protocols, and proper diabetic control are combined. Risk rises in revision cases and in patients with poorly controlled blood sugar. Severe infection may require temporary implant removal and replacement after the tissue clears. |
| Mechanical Failure | Below 5% in the first decade. Modern three-piece systems are engineered for 15 to 20 years, but pumps, tubing, and seals can wear over time. Failure is usually gradual rather than sudden, and revision surgery to replace the implant is straightforward. |
| Auto-Inflation | Rare with modern lock-out valve designs. Older implants occasionally inflated under abdominal pressure, but current AMS, Coloplast, and Rigicon pumps include safety mechanisms that prevent passive activation. |
| Cylinder Erosion | Rare, around 1% or less. Seen primarily in patients with severe corporal fibrosis, prior radiation, or spinal cord injury where sensation is reduced. Careful candidate selection and sizing during surgery minimize this risk significantly. |
| Persistent Pain | Mild discomfort during the first weeks is expected. Long-term persistent pain affecting daily life occurs in fewer than 3% of patients and is more common when implant sizing or placement is suboptimal. |
How Long Does an Inflatable Implant Actually Last?
Modern three-piece implants are engineered for 15 to 20 years of reliable function, and long-term data supports those numbers in real clinical practice. A 2025 study of 250 patients published in the Turkish Journal of Urology reported satisfaction rates of 92.4% after inflatable implant surgery, and the 10-year mechanical survival rate across the three major manufacturers sits above 80%.
Reliability differs by brand engineering. The AMS 700 shows 10-year mechanical survival above 85% in published series, with many devices functioning reliably past 15 years thanks to decades of clinical refinement and the established Tenacio pump system. The Coloplast Titan reports 10-year survival above 80%, with Bioflex cylinder material engineered for resistance to wear under repeated inflation and a lifetime device warranty for mechanical failure. The Rigicon Infla10 Pulse is newer to long-term data but is engineered to match competitor durability, with HydroShield coating, ergonomic pump design, four-layer cylinder construction, and a lifetime warranty included.
Warranty coverage is worth understanding before surgery. Coloplast and Rigicon both offer lifetime device replacement warranties on mechanical failure, while Boston Scientific provides time-limited coverage that varies by region. Warranty replaces the device itself, but surgery, hospital, and anesthesia costs for revision are generally not covered.
When mechanical issues do appear after many years of use, revision surgery is straightforward in experienced hands. The original incision is reopened, the failed component is removed, and a new implant is placed. Most revision cases are completed in a single operation with similar recovery to first-time surgery. The full revision process is covered in our Penile Implant Revision Surgery guide.
When Inflatable Is the Clear Choice
The choice between an inflatable and a malleable implant is rarely abstract. It comes down to specific situations in a patient’s life where one device fits and the other creates daily friction.
- Natural flaccid state between encounters
- Invisible under all clothing and swimwear
- On-demand control matches an active sex life
- Handles complex Peyronie’s with strong-rigidity cylinders
- 15 to 20 year engineered lifespan
- No pump operation required
- Easier through dense scar tissue
- Lowest long-term mechanical risk
- Simpler surgical path through scarred anatomy
- Better for patients with weak hand strength
The decision pattern is consistent. Active lifestyle, concealment priority, partner dynamics, and under-60 age usually point to an inflatable. Reduced hand function, complex pelvic anatomy, severe fibrosis, and a strong preference for mechanical simplicity usually point to a malleable. Specific anatomical situations also matter: prior radical prostatectomy or kidney transplant complicates reservoir placement, sometimes requiring a two-piece system. Severe corporal fibrosis sometimes makes a malleable the only feasible option.
The full clinical breakdown of the malleable indication, including the specific patient profiles where it genuinely outperforms an inflatable, is covered in our Malleable Penile Implant guide.
Frequently Asked Questions
During the first two weeks, sleeping on the back with supportive underwear is recommended to reduce pressure on the surgical site. After healing is confirmed at the 4 to 6 week follow-up, all sleeping positions are allowed and the implant does not restrict normal sleep.
Conclusion
The three-piece inflatable implant is the closest current medicine comes to restoring a natural erection cycle in men whose vascular and hormonal pathways no longer respond to treatment. Rigidity is on demand, deflation is real, and the entire system disappears into daily life within months of recovery. For the right candidate, the difference between living with severe ED and living after an inflatable implant is the difference between organizing life around erectile uncertainty and not thinking about it at all.
The inflatable is not the right device for every patient. Severe corporal fibrosis, reduced hand function, and specific anatomical limitations sometimes point in another direction. The first useful step is a medical evaluation that looks at anatomy, lifestyle, and long-term expectations rather than at advertised packages. From there, the right device and the right surgical plan become clear.
If you are considering an inflatable penile implant, a proper consultation reviews your medical history, current situation, and anatomical findings before any device is recommended. Patients with severe ED that no longer responds to medication, injection, or vacuum therapy are typically the strongest candidates, but the final answer depends on the individual clinical picture.