If you can get an erection but cannot hold it long enough to finish, you already know how this feels. The arousal works. The start works. Then within a minute or two, sometimes less, firmness drains away and the moment is over. After enough repetitions, the medication that used to help stops helping, and nobody seems to give you a clear answer for what is actually going wrong.
This is the pattern that brings most patients to a vascular evaluation years later than they should have had one. The diagnosis they should have received was never run. They were prescribed Viagra at progressively higher doses, told to relax, sometimes told the problem was in their head. In a small number of cases that is true. For most, the real cause is mechanical: blood enters the penis normally but escapes too quickly through the veins to keep an erection stable.
Venous leakage is a vascular cause of erectile dysfunction, and it does not respond to the standard treatment ladder the way ordinary ED does. Oral medications are designed to push more blood in. The problem in venous leakage is that the blood does not stay. Until that is confirmed with the right diagnostic test, every treatment is a guess.
This guide explains what venous leakage actually is in plain language, why it gets missed for years, why pills produce partial results at best, and what treatment options realistically work once the leak has been confirmed. By the end you should know what test to ask for, what to expect from each treatment option, and how to decide which path fits your situation.
- What Is Venous Leakage in the Penis?
- Symptoms of Penile Venous Leakage
- What Causes Penile Venous Leakage
- How Venous Leakage Is Diagnosed
- Why Pills Fail When the Problem Is Venous Leakage
- Non-Surgical Venous Leakage Treatment Options
- Surgical Venous Leakage Treatment
- Comparing Surgical Venous Leakage Treatment Options
- Slowing the Progression of Venous Leakage
- Venous Leakage Treatment: The Bottom Line
- What Is Venous Leakage in the Penis?
- Symptoms of Penile Venous Leakage
- What Causes Penile Venous Leakage
- How Venous Leakage Is Diagnosed
- Why Pills Fail When the Problem Is Venous Leakage
- Non-Surgical Venous Leakage Treatment Options
- Surgical Venous Leakage Treatment
- Comparing Surgical Venous Leakage Treatment Options
- Slowing the Progression of Venous Leakage
- Venous Leakage Treatment: The Bottom Line
Key Points
- Venous leakage is a vascular condition where blood enters the penis but cannot stay trapped long enough to maintain a stable erection.
- The signature symptom is an erection that starts firm and fades within minutes, regardless of arousal or stimulation.
- Penile Doppler ultrasound is the diagnostic test that confirms venous leakage and measures how severe it is.
- Oral medications like Viagra and Cialis produce partial results because they treat inflow, while venous leakage is an outflow problem.
- Realistic treatment options range from lifestyle changes and vacuum devices to penile implant surgery in confirmed advanced cases.
- Without a confirmed diagnosis, treating venous leakage is guesswork. The Doppler study should come first.
What Is Venous Leakage in the Penis?
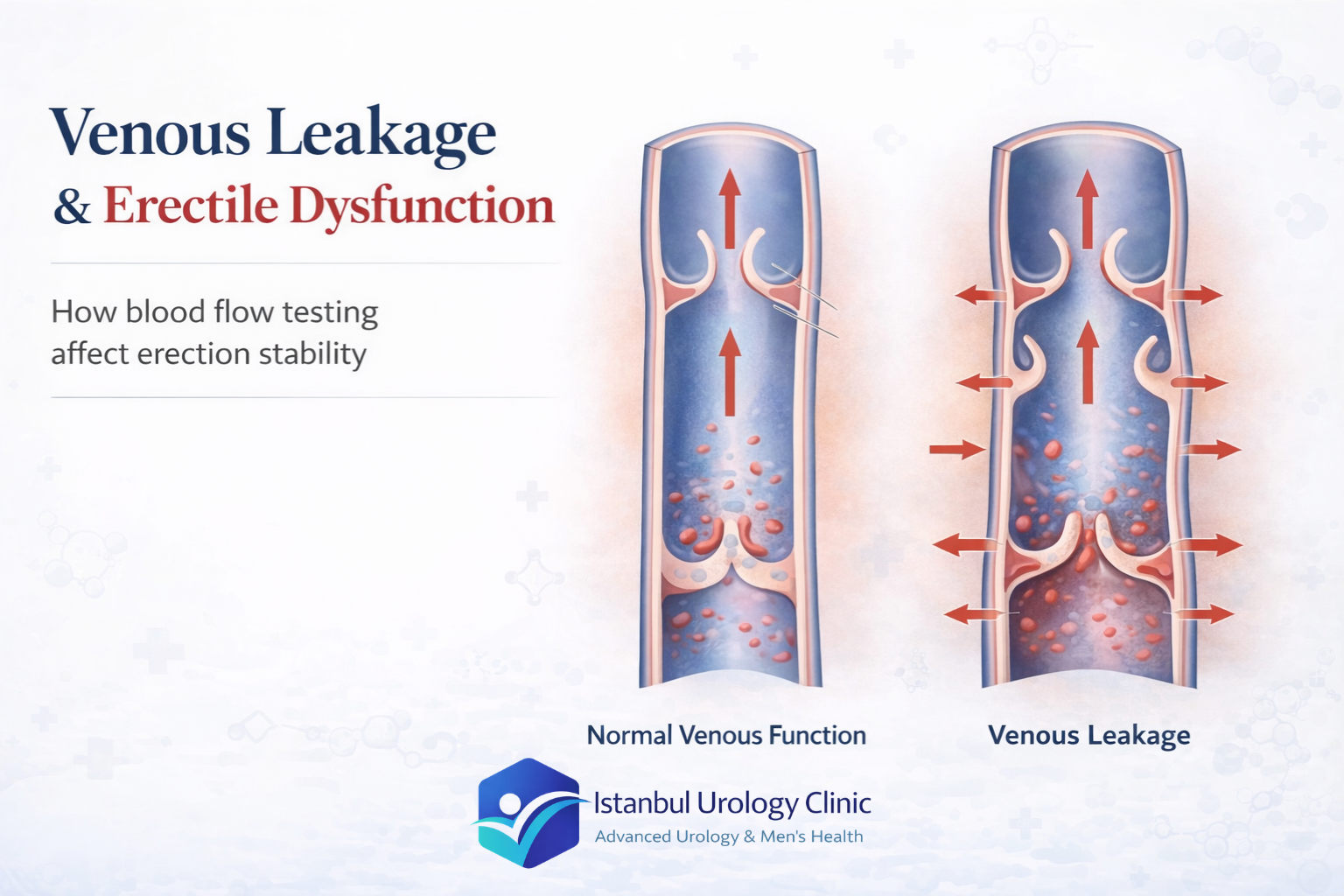
A normal erection depends on two mechanics working together: blood flowing in, and blood staying in. During arousal, the arteries deliver blood into the two erection chambers that run along the length of the penis. As these chambers fill, the penis expands and stiffens. At the same time, the outer covering of the penis presses on the veins that normally drain blood out, sealing them shut. That seal is what holds the erection in place.
Blood Flows In
Arteries deliver blood into the two erection chambers along the length of the penis. The chambers fill, and the penis becomes firm.
The Seal Activates
The outer covering of the penis compresses the veins that drain blood out. The veins close. Blood is now trapped inside.
The Erection Holds
As long as the seal works and arousal continues, pressure stays high and the erection is sustained throughout intercourse.
In venous leakage, step 2 fails. The seal does not work. The veins remain partly open, and blood drains out faster than the arteries can replace it. The erection may still start normally because the inflow side is intact. The problem appears within seconds or minutes, when pressure cannot be maintained and firmness collapses. This is why patients describe an erection that “arrives but will not hold,” even when arousal is strong and stimulation continues.
Venous leakage is one of the recognized vascular causes of erectile dysfunction, alongside arterial insufficiency. The two are sometimes confused because the surface symptom looks similar, but the underlying mechanism is opposite. Arterial insufficiency means not enough blood is getting in. Venous leakage means the blood that gets in cannot stay. Treatment for the two conditions is very different, which is why an accurate diagnosis matters more than the prescription that follows it.
The other important point: venous leakage is not always a permanent or untreatable condition. Mild cases can sometimes stabilize with lifestyle changes and vascular conditioning. Established cases usually need a more direct intervention. The right starting point in either case is confirming what is actually happening inside the penis during an erection, which the next section explains.
Symptoms of Penile Venous Leakage
The symptoms of venous leakage centre on one core problem: an erection that starts but does not hold. Arousal works. Initiation works. The breakdown happens later, when the pressure inside the penis cannot be maintained long enough to complete intercourse. The four patterns below cover what most patients describe when they first arrive.
| Symptom | What Patients Describe and Why It Matters |
|---|---|
| Difficulty Maintaining an Erection | The erection arrives normally, then fades within minutes or seconds despite continued stimulation. This is the signature complaint of venous leakage: the seal that traps blood inside the penis is failing, so pressure cannot be sustained long enough to complete intercourse. |
| Inconsistent Firmness | Firmness fluctuates during the same encounter: strong at first, then softer, then firm again. Partial venous outflow produces unstable pressure inside the penis rather than full loss, which is why many men question whether the cause is physical or psychological. |
| Reduced or Absent Morning Erections | The natural erections that happen during sleep and on waking weaken or disappear over time. Healthy morning erections are a reliable indicator of normal vascular function in the penis, so their loss points clearly toward a vascular cause rather than a situational one. |
| Short Erection Duration | Even with adequate arousal, the erection cannot be held long enough to complete intercourse. This pattern is the classic signature of venogenic erectile dysfunction, and it is precisely what a penile Doppler ultrasound is designed to confirm. |
The psychological dimension should not be underestimated. Repeated episodes erode confidence quickly, and the performance anxiety that follows compounds the physical problem, making erections harder to maintain even when blood flow is partially adequate. By the time most patients reach a vascular workup, they are carrying both the underlying vascular issue and the emotional weight it has built up over months or years.
What Causes Penile Venous Leakage
| Cause | How It Damages the Vein Seal |
|---|---|
| Aging | Blood vessels lose elasticity gradually. The veins inside the penis become less able to close during an erection, allowing blood to escape before pressure stabilizes. The change is slow and often unnoticed until the problem is well established. |
| Diabetes & Cardiovascular Disease | Both conditions cause progressive vascular damage throughout the body. The same vessel changes that affect systemic circulation affect penile blood flow, making a stable erection increasingly difficult regardless of arousal. |
| Peyronie’s Disease | Scar tissue inside the penis distorts the outer covering responsible for compressing the draining veins during an erection. Once that structural integrity is lost, the seal fails. Venous leakage is a well-documented complication of Peyronie’s. |
| Low Testosterone | Testosterone supports vascular tone and smooth muscle function in the penis. When levels drop below the threshold needed for normal erectile physiology, the tissue changes that follow reduce the penis’s ability to trap blood. Rarely the sole cause, but a frequent contributor. |
| Pelvic Trauma & Surgery | Injury to the pelvic region or surgical procedures involving the prostate can damage the nerves and blood vessels that coordinate erection. Depending on the extent of damage, venous leakage can develop as a direct consequence. |
| Smoking, Alcohol, Inactivity | Smoking accelerates vascular damage by restricting blood flow and damaging vessel walls. Excessive alcohol disrupts hormones and nerve signalling. Inactivity compounds both. These habits worsen the underlying vascular environment that makes venous leakage more likely. |
How Venous Leakage Is Diagnosed
Venous leakage is suspected when a man can achieve an erection initially but loses it quickly, or when oral medications such as Viagra and other pills like it deliver partial or inconsistent results. The evaluation begins with a complete medical history, focusing on diabetes, vascular disease, neurological conditions, and pelvic trauma, all of which raise the probability of a vascular cause. A physical examination follows, checking for structural changes in the penis, including signs of Peyronie’s disease.
One of the most useful early distinctions is between venous leakage and psychological erectile dysfunction, because they can look similar on the surface. Men with psychological ED usually maintain normal morning erections, and their difficulties tend to appear in specific situations or with particular partners. Men with venous leakage lose erections consistently, regardless of context, and their morning erections are frequently weak or absent. The pattern matters, but the pattern alone is not the diagnosis.
This distinction is also reflected in the European Association of Urology’s Sexual and Reproductive Health Guidelines, which classify venous leakage among the vasculogenic causes of erectile dysfunction and recommend penile Doppler ultrasound as the standard non-invasive investigation when a vascular cause is clinically suspected.

The Test That Confirms Venous Leakage
The standard first-line investigation is a penile Doppler ultrasound. The study measures how blood flows into the penile arteries and how effectively the veins retain that blood during a controlled erection. It is the only widely available test that can directly distinguish an outflow problem from an inflow problem, which is the central question in any vascular ED workup.
For a full explanation of how the Doppler study is performed, what to expect during the appointment, and how the results are read, see our complete guide to penile Doppler ultrasound. The short version: the test is non-surgical, takes under 40 minutes, requires no anaesthesia, and produces a definitive answer in most cases.
Where a more detailed anatomical picture is needed, cavernosography (an imaging study using contrast dye) and dynamic infusion cavernosometry (a pressure-based assessment) are available. Both are reserved for select cases where the Doppler result is borderline or surgical planning requires additional precision. They are not part of routine evaluation. Blood tests are also ordered, usually covering testosterone, cholesterol, and blood glucose, to assess the broader vascular and hormonal picture.
The reason diagnosis matters so much here is practical. Treating venous leakage without confirming it first means treating an assumption. The treatment pathways for venous leakage, arterial insufficiency, and psychological ED diverge sharply after this point. Getting the diagnosis right is what makes the rest of the treatment plan worth the effort.
Why Pills Fail When the Problem Is Venous Leakage
Most patients who reach a vascular evaluation for venous leakage have already spent months, often years, working through the standard pharmacy options. Viagra. Cialis. Sometimes Levitra or generic equivalents at progressively higher doses. The pattern is almost identical: the medication produces a noticeable effect at the start, the erection arrives, then it fades anyway, regardless of dose, timing, or stimulation.
That outcome is not a personal failure or a sign that the medication is fake. It is a structural mismatch between what these drugs do and what venous leakage actually is.
The Inflow Problem vs the Outflow Problem
Pills like Viagra (sildenafil) and Cialis (tadalafil) work by relaxing the smooth muscle of the penile arteries and increasing how much blood flows in. They are inflow medications. They are highly effective when the problem is reduced arterial supply, which is the case in many men with mild to moderate erectile dysfunction.
Venous leakage is the opposite problem. The arteries are doing their job. Blood enters the penis normally. The failure is on the outflow side: the veins that should close to trap that blood are leaking it out faster than the arteries can replace it. Pouring more water into a bucket with a hole in the bottom does not fill the bucket. It just makes the leak more obvious.
Arteries fail to deliver enough blood into the erection chambers. The seal works, but there is not enough volume to fill the penis firmly. Pills like Viagra and Cialis open the arteries, allowing more blood to reach the chambers, and the erection develops as expected.
Typical response to pills: Reliable. Predictable. The medication does exactly what it is designed to do.
Blood enters the penis normally, but the veins fail to close and trap it. The chambers fill, then drain. Pushing more blood in through inflow medication does not change the fact that the seal is broken. The erection arrives, then fades, sometimes within seconds of penetration.
Typical response to pills: Partial. Inconsistent. Dose-resistant. Higher doses extend the effect by a minute or two and add side effects, but the leak is unaffected.
What This Looks Like in the Bedroom
The clinical picture is consistent across patients. A man takes 50 or 100 milligrams of sildenafil an hour before intercourse. The erection arrives on schedule. Penetration is possible. Within two to five minutes, firmness begins to decline. Some men describe needing to stop and restart. Others describe the erection collapsing entirely partway through.
Doubling the dose to 200 milligrams might extend the window by a minute or two but introduces side effects (headache, flushing, nasal congestion, visual disturbances) without solving the core issue. By the time these patients reach us, many have also tried injection therapy with medications like alprostadil or trimix. Injections produce a stronger erection in most men with vascular ED. For venous leakage specifically, the injection-induced erection is more robust, but the leak is still there. The erection holds longer, but not the way a normal erection should, and patients describe the experience as functional rather than natural.
Why More Medication Is Not the Answer
Patients sometimes ask whether the solution is simply more medication. The honest answer is no. Going from 50 to 100 milligrams of sildenafil produces a real benefit for many men with ED. Going from 100 to 200 milligrams produces diminishing returns and rising side effects. None of these dose increases address what is structurally wrong with the penile veins. They are pushing harder on a system that is leaking.
A man on maximum doses of oral medication who still cannot complete intercourse has reached the ceiling of what inflow medication alone can deliver. The next step is not another prescription. It is the diagnostic test that confirms what is actually happening to the blood once it enters the penis. In men with mild vascular ED, pills produce a clear and sustained response. In men with venous leakage, the response is partial, inconsistent, and dose-resistant. That alone is often enough to raise the suspicion of an outflow problem and proceed directly to a Doppler study.
If three or more of these patterns describe your situation, the issue is unlikely to be solved by another prescription. A Doppler study should be the next step before any further treatment decision.
- Erections begin firm and fade within minutes, despite continued arousal
- Morning and night-time erections have become weak or have stopped
- Oral medications worked at first and have become less reliable over time
- Higher doses produce more side effects but no real improvement in duration
- You can reach an erection through stimulation but cannot maintain it during intercourse
- Penetration is possible but firmness collapses partway through
Non-Surgical Venous Leakage Treatment Options
Treatment for venous leakage usually starts conservatively. The reasoning is straightforward: the more invasive the intervention, the more it should be reserved for cases where less invasive options have been tried or ruled out. The table below summarizes the realistic non-surgical options, what each one does mechanically, and who tends to benefit. None of them close a venous leak permanently, but several are useful at different stages or alongside other treatments.
| Option | How It Works | Realistic Outcome | Best Suited For |
|---|---|---|---|
| Lifestyle Changes | Exercise, weight loss, smoking cessation, controlled alcohol intake, and better management of diabetes or blood pressure. Improves overall vascular health and slows further deterioration. | Modest improvement in early or mild cases. Limited effect once leakage is established. | Younger men, early cases, anyone with reversible vascular risk factors. |
| Oral Medications (Viagra, Cialis) | Increase blood flow into the penile arteries. Designed to improve inflow, not to fix outflow. | Partial, inconsistent response. The erection becomes firmer at the start but still fades. | Patients with mild leakage who may benefit from a combined approach. Often disappointing as a standalone treatment. |
| Vacuum Erection Device | A pump draws blood into the penis mechanically. A constriction ring at the base traps the blood and holds the erection. | Produces a usable erection in most men. The ring is the workaround for the leak, not a treatment for it. | Men who prefer a non-pharmaceutical, non-surgical option and are comfortable with the device. |
| Hormone Replacement (Testosterone) | Corrects low testosterone where it is measured and confirmed. Supports vascular tone and smooth muscle function in the penis. | Useful when low testosterone is a real contributor. Not a treatment for venous leakage on its own. | Men with documented low testosterone alongside their venous leakage. |
| Stem Cell / Regenerative Therapy | Injection-based approach that aims to support vascular and erectile tissue regeneration. Results vary widely between patients. | May help in some early cases. Not currently a definitive treatment, and not appropriate for advanced leakage. | Carefully selected patients in early-stage disease. Read more in our guide to stem cell injection for erectile dysfunction. |
| Psychological Support | Counselling and sex therapy address the performance anxiety and relationship strain that often build on top of a physical problem. | Does not treat the vascular issue but can meaningfully reduce the secondary anxiety layer. | Any patient where confidence and anxiety have become part of the problem, which is most patients with longstanding venous leakage. |
The honest summary: non-surgical options manage the problem rather than solve it. For a man in his thirties with a mild, recently identified leak and modifiable lifestyle factors, conservative treatment is the right starting point. For a man who has already spent years on pills and injections without adequate results, the conversation usually needs to move toward a more definitive solution.
Surgical Venous Leakage Treatment
When conservative treatments have been exhausted without adequate results, the conversation moves to surgical options. Three approaches exist. They differ substantially in their mechanism, their durability, and the type of patient they suit. Understanding the difference matters because the wrong procedure for the wrong patient is a common pattern in venous leakage care globally.
The three approaches also represent a clinical progression: from procedures that try to repair the leaking veins (limited durability) to a procedure that bypasses the venous system entirely (the most reliable long-term option). The timeline below maps that progression.
Venous Embolization
A minimally invasive procedure performed by interventional radiology. A thin catheter is guided into the penile venous system, and blocking material is deployed directly into the leaking veins. The goal is to stop premature drainage without open surgery. Results are inconsistent, the procedure is not widely available, and long-term data remain limited. For carefully selected patients with an anatomically accessible leak, it is reasonable to discuss. For most patients with established venous leakage, it is not a durable fix.
Venous Ligation Surgery
Open surgical closure of the veins that allow blood to drain from the penis prematurely. The procedure was performed more frequently in the past. Its decline is straightforward to explain: the penis has a complex venous network, and when one pathway is closed, the body develops alternative drainage routes over time. Short-term improvement is documented in a proportion of patients, but long-term outcomes decline consistently as collateral veins form. Most experienced prosthetic urologists today reserve this procedure for a narrow group of younger patients with isolated, anatomically discrete leakage.
Penile Implant Surgery
A medical device is placed inside the erection chambers, allowing the patient to achieve a firm, controlled erection on demand. Unlike the previous two approaches, the implant does not try to repair the leaking venous system. It bypasses it entirely. The venous leak becomes irrelevant because the device creates rigidity mechanically, independent of blood trapping. For patients with confirmed advanced venous leakage who have spent years managing a condition that responds poorly to everything else, this is the most reliable long-term solution available today.
The specific implant chosen depends on anatomy, medical history, and patient preference. Our practice routinely uses three platforms: the AMS 700 from Boston Scientific, the Coloplast Titan, and the Rigicon Infla10 AX. The decision between them is made during the surgical consultation based on the clinical picture. Full details on each platform and how implants work mechanically are covered in our complete penile implant surgery in Turkey guide.
Comparing Surgical Venous Leakage Treatment Options
The three surgical approaches differ in how they attempt to solve the leak, how durable the result is, and which patients are good candidates. The table below summarizes the trade-offs that matter most when making this decision.
| Factor | Venous Embolization | Venous Ligation Surgery | Penile Implant Surgery |
|---|---|---|---|
| How It Works | Catheter-guided blocking of leaking veins from inside the venous system. | Surgical closure of the veins responsible for premature blood drainage. | A device is placed inside the erection chambers to create rigidity mechanically, bypassing the leak entirely. |
| Mechanism Target | Closes the leak itself. | Closes the leak itself. | Bypasses the leak. The venous system becomes irrelevant. |
| Invasiveness | Minimally invasive, interventional radiology. | Open surgical procedure. | Surgical procedure under general anaesthesia. |
| Long-Term Results | Inconsistent. The body forms new drainage pathways over time, and symptoms often return. | Initial improvement in some patients, declining steadily as collateral veins form. | Highly reliable. Device survival 96% at 5 years, 86% at 10 years. |
| Best Candidate | Selected patients with an anatomically discrete, accessible leak. | Narrow group of younger patients with isolated, well-defined leakage. | Patients with advanced venous leakage who have not responded to other treatments. |
| Availability | Limited. Performed in specialised centres only. | Rarely performed today. Most prosthetic urologists have moved away from it. | Widely available at experienced urology centres, including ours. |
| Reversibility | Difficult to reverse once veins are embolized. | Not reversible. | The device can be removed or replaced if needed. |
| Clinical Verdict | Reasonable to discuss in select cases. Not a durable fix for most. | Historical procedure. Reserved for a narrow patient profile. | The most reliable long-term solution for confirmed advanced venous leakage. |
The pattern is clear when the options are placed side by side. Embolization and ligation both attempt to repair a venous system that has already proven unable to do its job, and the body’s tendency to develop alternative drainage routes works against both.
Penile implant surgery takes a different approach: it does not try to fix the vascular problem, it removes the dependency on it. For patients with confirmed advanced venous leakage and a history of failed conservative treatments, this is why it has become the standard recommendation in experienced prosthetic urology practice.
Slowing the Progression of Venous Leakage
Venous leakage cannot always be prevented, particularly when the underlying cause is aging, congenital weakness, or scarring from Peyronie’s disease. The vascular deterioration that drives most cases can be slowed, and in some early situations meaningfully reversed, through consistent lifestyle changes. These are not generic wellness recommendations. Each has a direct mechanism that affects penile blood flow.
Regular Physical Activity
Exercise improves vascular tone throughout the body, including the blood vessels of the penis. Pelvic floor training supports the muscles that assist erection. Aim for 30 minutes of moderate activity most days. Consistency matters more than intensity.
Balanced Diet
What damages blood vessels systemically damages penile blood vessels too. Build meals around vegetables, fruit, whole grains, legumes, and lean protein. Processed foods and high-sugar diets accelerate the vascular changes that drive venous leakage.
Quitting Smoking
Smoking attacks the inner lining of blood vessels and restricts penile blood flow. Among all the lifestyle factors linked to erectile dysfunction, stopping smoking produces some of the most measurable vascular improvements.
Limiting Alcohol
Alcohol disrupts hormone levels and circulatory function. The often-quoted “two drinks per day” is a ceiling, not a target. Men already experiencing erectile difficulties usually see better outcomes by reducing consumption further.
Managing Chronic Conditions
Diabetes, hypertension, and high cholesterol are the most consistent drivers of penile vascular damage. Active medical management, rather than tolerating suboptimal control, protects long-term erectile function. The damage these conditions cause accumulates silently before symptoms appear.
Managing Stress
Chronic stress keeps cortisol elevated, constricting blood vessels and suppressing the hormonal environment for normal erectile function. It also creates the performance anxiety that compounds any underlying physical problem. Exercise, structured relaxation, and addressing chronic stressors all help.
Frequently Asked Questions
Yes. Although it is more common in older men with vascular disease, venous leakage does occur in younger patients, sometimes from a congenital weakness in the venous system, sometimes from pelvic trauma, hormonal disruption, or early vascular abnormalities. Persistent ED in a young man should not be assumed psychological before a proper vascular evaluation has ruled out a physical cause.
Mild, early venous leakage can sometimes stabilize with aggressive lifestyle changes and treatment of underlying conditions like diabetes. Established venous leakage does not resolve on its own. The structural problem in the venous system does not repair itself once it has developed.
Venous leakage is a mechanical problem, not a hormonal or psychological one. Desire is usually preserved, which is part of what makes the condition so frustrating. The will is there, the body cannot deliver. Over time, repeated failures can erode confidence and indirectly affect desire, but the primary problem is vascular.
Partially, at best. Viagra, Cialis, and similar medications increase blood flow into the penis. Venous leakage is an outflow problem. Pushing more blood into a system that cannot hold it produces a firmer start but the erection still fades. This is the typical pattern most patients describe.
Yes, with penile implant surgery in advanced cases. The implant bypasses the leaking venous system entirely, creating rigidity mechanically rather than relying on blood trapping. This is the most reliable long-term solution and the standard recommendation when conservative options have been exhausted.
Penile Doppler ultrasound is the primary diagnostic test. It measures arterial inflow and venous retention directly and confirms whether the problem is outflow rather than inflow. A full explanation of what to expect during the test is in our guide to penile Doppler ultrasound.
Yes, particularly when the underlying causes (diabetes, smoking, untreated cardiovascular disease) are not addressed. The vascular deterioration is progressive. Many patients describe a pattern where medications worked at first, became less reliable over a year or two, then stopped working entirely.
Yes, the erection usually arrives. The problem is holding it. Patients with venous leakage typically report a firm start, then a rapid loss of firmness within seconds or minutes of penetration. The arousal and initiation phases are intact. The maintenance phase fails.
Exercise improves vascular health generally and may slow the progression of venous leakage in early cases. It does not close an established leak. Where vascular risk factors like obesity, diabetes, and poor cardiovascular fitness are present, addressing them is part of any responsible treatment plan, but exercise on its own is not a treatment for confirmed leakage.
Yes. Some blood pressure medications, antidepressants, and prostate medications carry erectile dysfunction as a known side effect. If symptoms began around the time a medication changed, raise it with the prescribing doctor before assuming a vascular cause. The simplest explanation should be ruled out first.
Venous Leakage Treatment: The Bottom Line
Penile venous leakage is a recognized vascular cause of erectile dysfunction. The problem is straightforward in its mechanism: blood enters the penis but cannot stay long enough to maintain a firm erection. The causes range from aging and chronic disease to structural changes from Peyronie’s, hormonal factors, and lifestyle-related vascular deterioration.
Diagnosis drives everything. A penile Doppler ultrasound identifies the problem directly and shows how advanced it has become. From there, treatment follows logically: conservative options first where they make sense, and more definitive options when the evidence points that way. Treating venous leakage without that foundation wastes time and produces poor results.
What to Do Next
- If pills worked at first and have lost their effect: request a penile Doppler study before any further dose increase.
- If a leak is confirmed and is early-stage: start with lifestyle changes and address vascular risk factors aggressively. Combine with oral medication where useful.
- If a leak is confirmed and is advanced: penile implant surgery is the most reliable long-term solution. The conversation should focus on which implant suits your anatomy and lifestyle.
- If you have not been evaluated yet: an honest diagnostic workup is the right starting point, regardless of which treatment path follows.
For the broader picture of how venous leakage fits into other vascular and non-vascular causes of ED, see the complete guide to erectile dysfunction treatment. The earlier the vascular cause is confirmed, the more options remain on the table.