Not every man who leaks after prostate removal is ready for an artificial urinary sphincter immediately. The first question is always whether the body still has room to recover on its own.
In the months following prostate removal, the neurological and muscular structures involved in urinary control are still adapting. Many patients regain meaningful continence during this period, particularly those who commit to consistent pelvic floor training. Operating too early means intervening before that natural recovery has had a chance to complete. We wait.
When leakage persists beyond that recovery window without measurable improvement, the evaluation shifts. At that stage, we are no longer waiting. We are assessing whether surgical restoration is appropriate. That assessment centers on three things.
The first is pad count. Three or more pads per day, consistently, indicates moderate to severe incontinence. One or two on difficult days is a different picture from three or more as a baseline.
The second is leakage pattern. Leakage triggered only by coughing or heavy lifting reflects a different level of sphincter weakness than leakage that occurs while walking, standing, or at rest. The pattern tells us how much closing function remains.
The third is response to conservative treatment. If structured pelvic floor rehabilitation has produced no meaningful improvement, muscle weakness alone is not the full explanation. Something more is driving the incontinence.
The typical candidate for an artificial urinary sphincter has undergone radical prostatectomy, has had sufficient recovery time without adequate improvement, has no severe uncontrolled bladder dysfunction complicating the picture, and retains enough hand dexterity to operate the device pump independently.
Selecting the right patients for an artificial urinary sphincter matters as much as the surgery itself. There are situations where implanting the device would be the wrong decision, and identifying those situations early is part of getting the outcome right.

Men with poorly controlled neurogenic bladder dysfunction are not suitable candidates. When the primary problem is the bladder itself rather than the urethral closing mechanism, placing a sphincter device does not address the actual pathology. Bladder function must be stabilized before any surgical implant is considered.
Significant cognitive impairment is another disqualifying factor. Operating the device requires the patient to understand when and how to activate the scrotal pump. If that understanding is not reliably present, the device cannot be used safely or consistently.
Hand dexterity matters for the same reason. The pump sits in the scrotum and must be compressed manually to allow urination. Patients with limited hand function due to neurological conditions, arthritis, or other causes may find independent use difficult or impossible.
Any active urinary tract infection must be fully resolved before surgery. Implanting a device into an infected field increases the risk of device infection substantially, and a device infection almost always means explantation. Surgery is postponed until the infection has cleared completely.
For men with mild stress urinary incontinence, particularly leakage triggered only by exertion, a male sling is often a more appropriate first intervention. It is a less complex procedure suited to less severe incontinence, and for the right patient it produces good results without the mechanical demands of a full sphincter device.
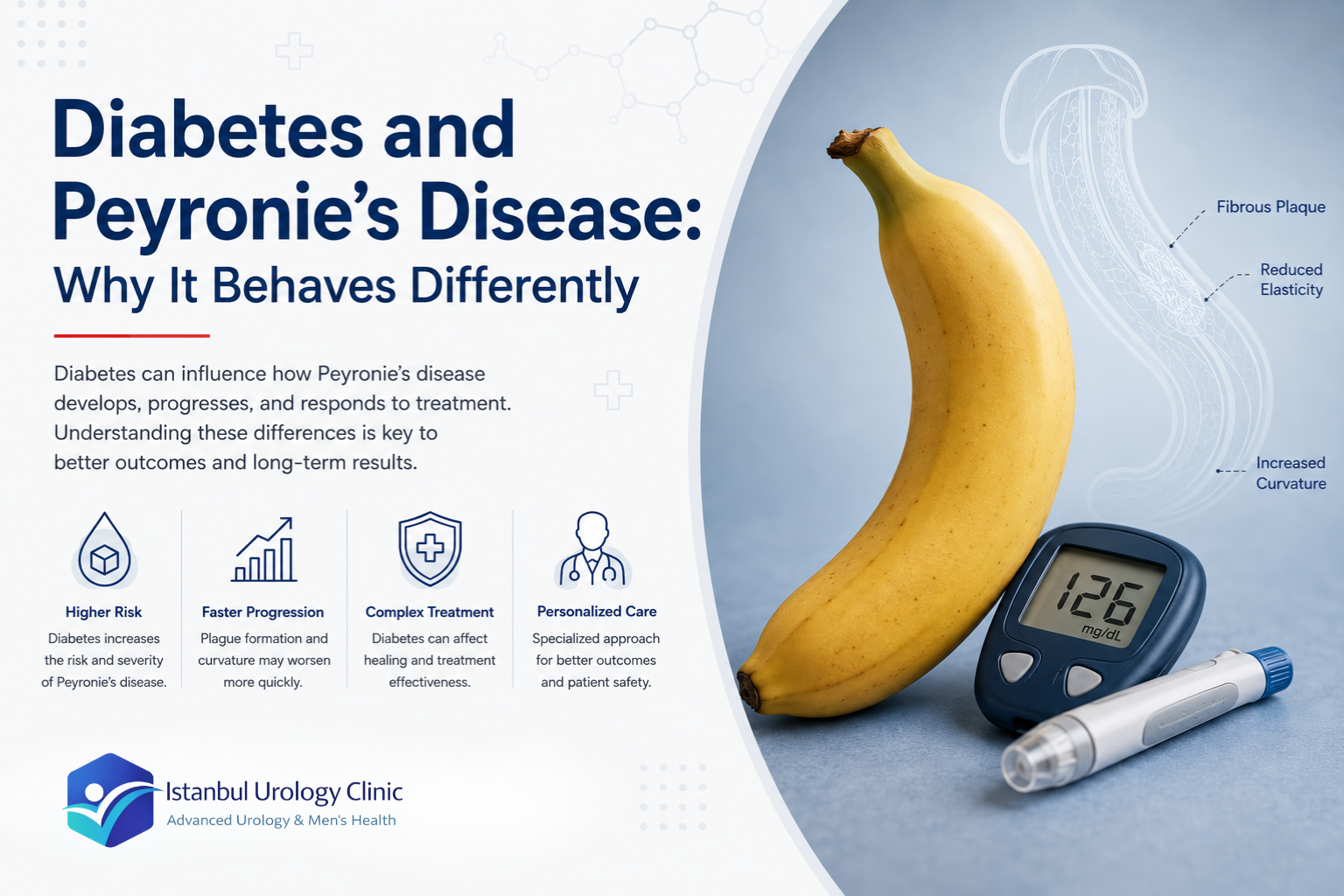
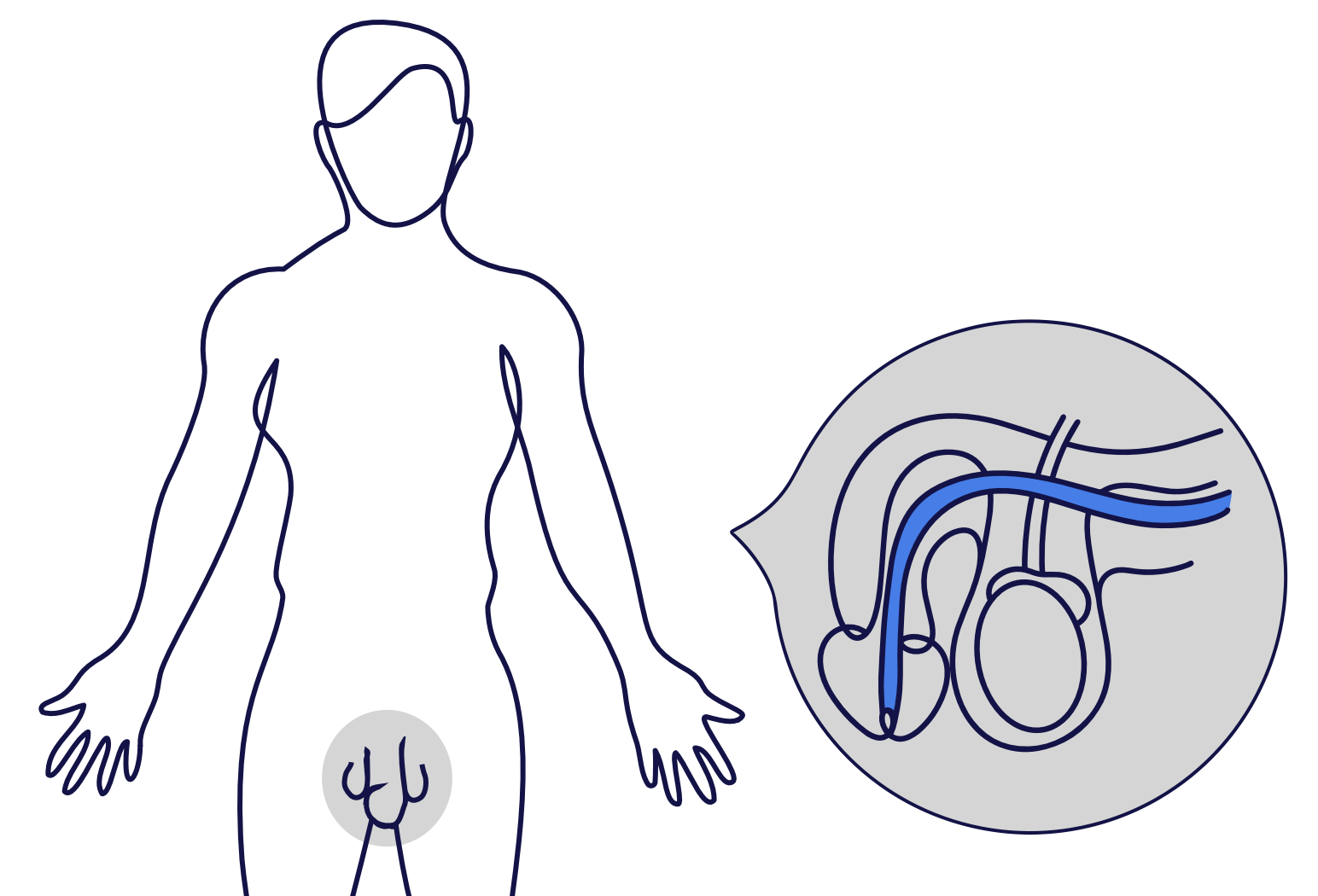
After prostate removal, the bladder itself usually continues to function normally. What changes is the closing mechanism. The natural sphincter muscle that kept the urethra sealed weakens during surgery, and without that valve, urine escapes during everyday activity: walking, standing, coughing, lifting.
The bladder is not the problem. The issue is the loss of the natural seal that keeps urine contained. The artificial urinary sphincter is designed to replace that seal mechanically. It does not alter bladder function, does not interfere with the nerves that signal the urge to urinate, and does not change the sensation of needing to go. It simply recreates the closing function the surgery disrupted.
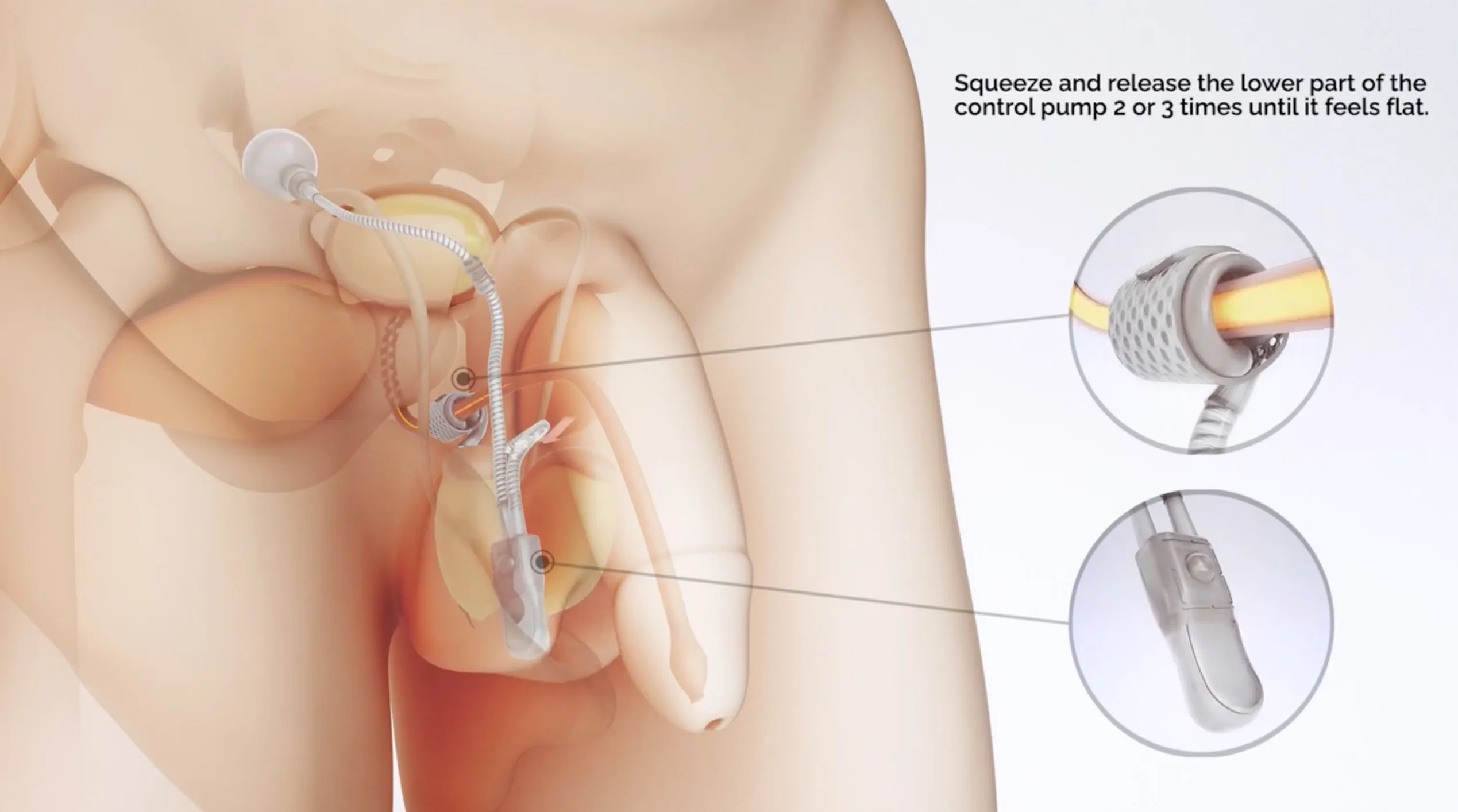
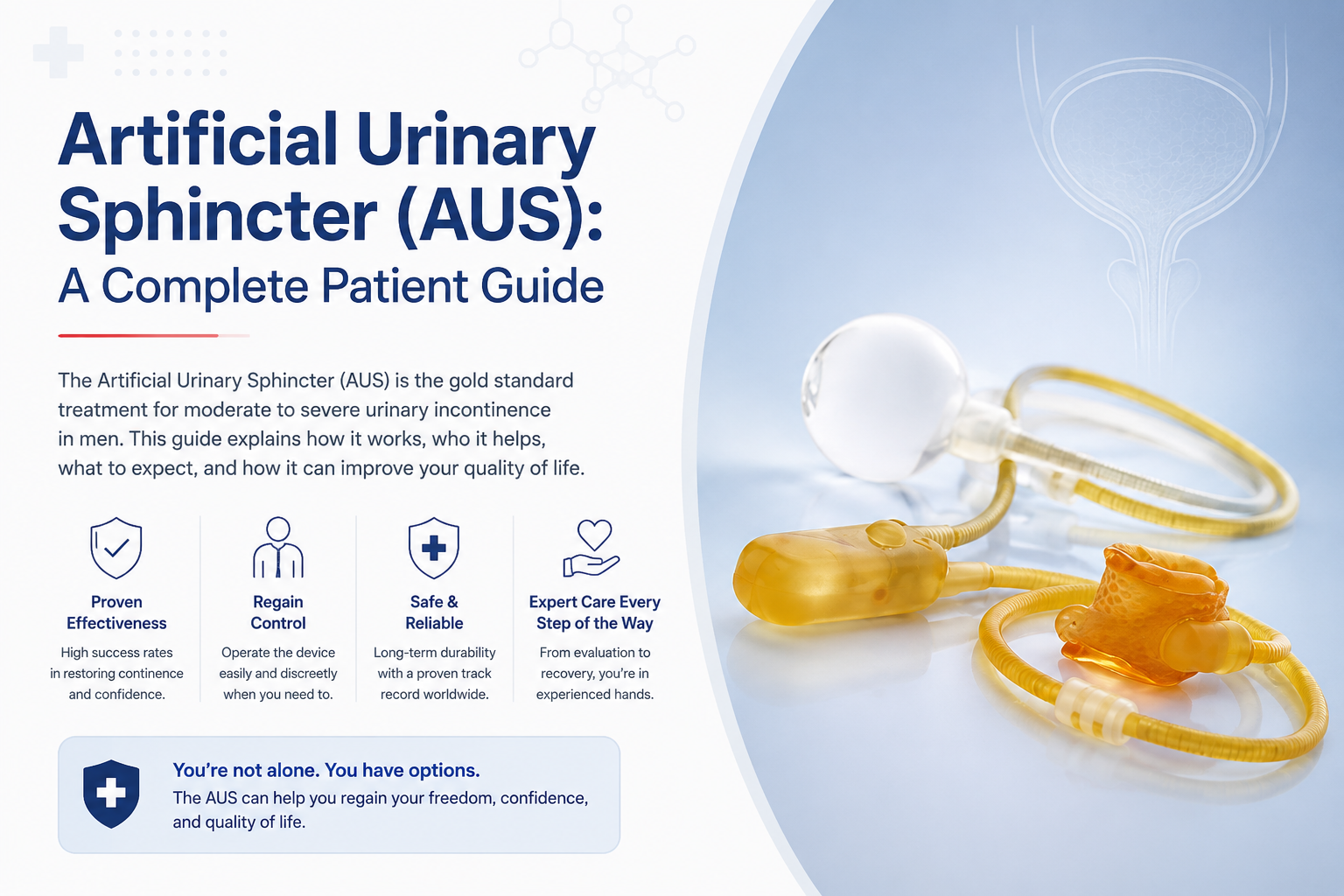
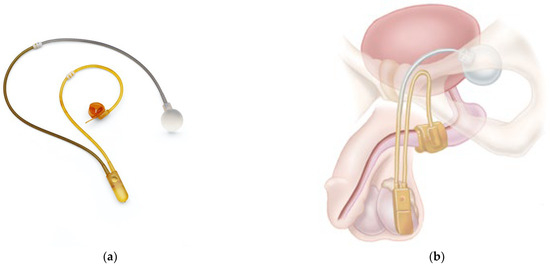
The device operates as a closed fluid system with three components:
- The cuff is a soft silicone band placed around the urethra. When fluid fills the cuff, it applies controlled pressure that keeps the urethra closed and prevents leakage between urinations.
- The scrotal pump sits inside the scrotum, invisible from the outside and positioned where the patient can reach it easily with his fingers. Pressing the pump is the only action required to urinate.
- The pressure-regulating balloon is placed in the lower abdomen. It maintains the correct fluid pressure throughout the system and ensures the cuff applies consistent, appropriate force without over-compressing the urethra.
When the patient needs to urinate, he squeezes the scrotal pump for a few seconds. Fluid transfers from the cuff into the balloon, the cuff opens, and urine passes normally. After one to two minutes, the fluid returns to the cuff automatically. The urethra closes again without any further action from the patient.
The urge to urinate remains completely intact, because the device works at the urethra, not the bladder. The sensation is normal. The timing is controlled by the patient. The closing happens on its own.
Surgical planning for an artificial urinary sphincter starts long before the procedure itself. The implant is not standardized. Cuff size, placement position, and surgical approach all depend on the individual anatomy and medical history of each patient.
Pre-operative evaluation focuses on the urethral tissue directly. Our team assesses thickness, elasticity, scarring from previous surgeries, and whether radiation therapy has been part of the patient’s cancer treatment. These factors determine where the cuff can be safely placed and how much pressure the surrounding tissue can tolerate over the long term.
The central surgical challenge is calibration. The cuff must compress the urethra enough to prevent leakage during daily activity, but not so much that it damages the tissue over time. That balance is what makes cuff placement the most technically demanding part of the procedure, and the part where experience has the greatest influence on outcome.
Once the cuff is positioned around the urethra, it is connected to the pressure-regulating balloon placed in the lower abdomen. The scrotal pump is then positioned where the patient can reach it comfortably with his fingers. The routing and positioning of each component is planned so the system functions smoothly in daily use without causing discomfort.
Patients who have received radiation therapy require additional surgical care. Irradiated tissue is less resilient, more prone to erosion, and carries a higher risk of complications if the cuff is placed without accounting for those changes. The technique adjusts accordingly, but the threshold for what the tissue can withstand is lower, and that has to be respected. The European Association of Urology guidelines recommend artificial urinary sphincter implantation as the preferred surgical option for moderate to severe post-prostatectomy stress incontinence.
A completed surgery is not the measure of success. The measure is a device that activates correctly, controls continence reliably, and continues functioning safely for years without revision.
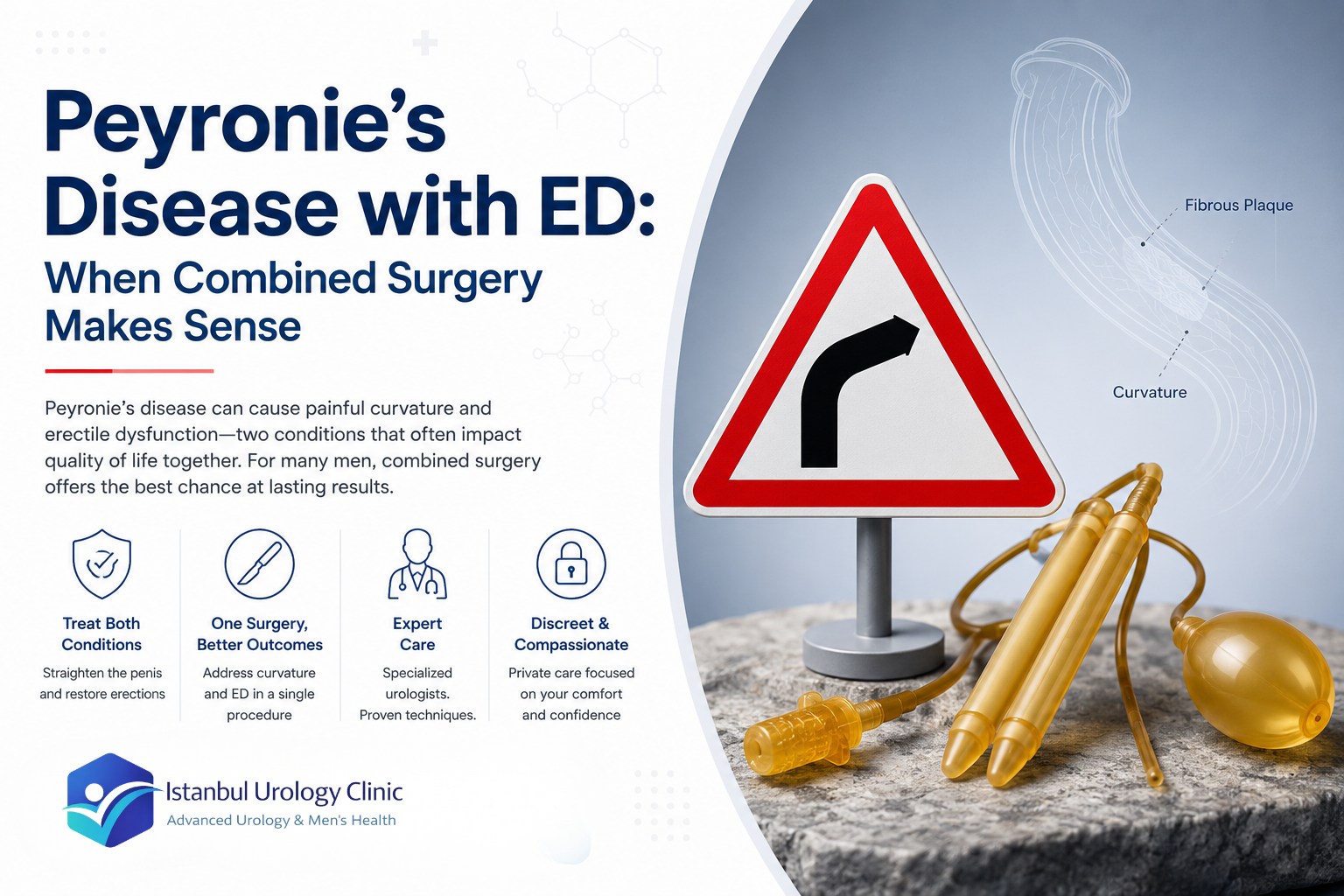
Prostate removal surgery can affect two separate functions simultaneously: urinary control and erectile function. The nerves responsible for erection run alongside the prostate, and surgical damage to those nerves is common. When both problems are present, treatment planning requires a different approach than managing either condition in isolation.

The central question is not simply how to treat the leakage, but whether both conditions should be addressed within the same treatment plan. When leakage is present throughout the day, during walking, standing, sitting, and sexual activity, a penile implant alone does not solve the problem. It restores erectile function. It does not control urine loss. Treating only one problem while leaving the other unaddressed produces an incomplete result.
When both problems are confirmed, the most complete solution is to treat them together. An artificial urinary sphincter manages urinary control, while a penile implant restores erectile function.
The two devices occupy different anatomical territories, one around the urethra and one inside the erectile chambers, which means they can be implanted without mechanical interference when the surgical planning is done correctly. The recovery curve, rehabilitation protocol, and decision points for erectile dysfunction after prostate surgery are covered separately in our complete guide to erectile dysfunction after prostatectomy.